Symptoms point to Parkinson’s
DEAR DR. ROACH: I am an 88-year-old widower. I live alone, care for myself, drive, and consider myself healthy. I take five prescription meds and seven over-the-counter meds, three of which were strongly recommended by doctors. I have diabetes and had a triple bypass surgery seven years ago.
I am writing because in 2024, I began having auditory and olfactory hallucinations. The auditory hallucinations have mostly been the sound of doors or cabinets closing. The olfactory ones range from perfume, to freshly baked goods, to smoke, peppermint, and an obnoxious chemical smell.
My primary care physician referred me to a neurologist, who ordered an MRI of my brain. It showed no tumors or evidence of stroke. The neurologist advised me to simply ignore the hallucinations if they continued.
My self-diagnosis is possible Lewy body dementia (LBD) since I have some mild Parkinson’s symptoms. Both the neurologist and the primary care physician have assured me that I do not have Parkinson’s or LBD. I don’t think that ignoring my hallucinations is good advice. Your opinion?
• R.L.R.
ANSWER: The combination of auditory and olfactory hallucinations is suggestive of a neurological disorder, such as Parkinson’s disease (PD) and the closely related LBD. You are right to be concerned. (I am also very impressed with your research skills and deductive powers.)
I am honestly surprised that the neurologist did not bring up these possibilities since phantosmia (smelling odors that aren’t there) is a well-recognized symptom of PD that can show up before abnormalities in the muscles. Approximately 10% of people with PD will have auditory hallucinations (hearing noises that aren’t there).
Getting an MRI was a good idea since tumors and strokes can sometimes cause these symptoms, and it’s good news that you don’t have one of these. But I remain puzzled as to why they seem adamant that you don’t have PD when you have symptoms of PD along with these hallucinations.
There is a treatment for hallucinations associated with PD, called pimavanserin. A visit to a neurologist with special expertise in PD (a movement disorder neurologist) would be helpful to see if you have PD or LBD and to consider treatment. It may be that your current symptoms are not causing you distress and that the risks of treatment may outweigh the benefit, but this is a decision that takes expertise and judgment. It is a decision that you should be a part of, which is why I recommend a neurologist with special expertise.
Lifestyles
Should I keep encouraging my parents’ divorce?
DEAR ANNIE: I have never been ignorant to the fact that, in my opinion, my parents’ marriage sucks. My dad is and ...
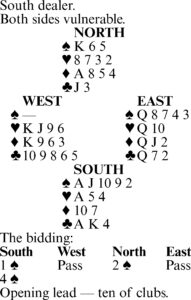
Bridge by Steve Becker
This hand occurred in a multiple team-of-four match. At most tables, West opened with a spade despite holding only ...
Symptoms point to Parkinson’s
DEAR DR. ROACH: I am an 88-year-old widower. I live alone, care for myself, drive, and consider myself healthy. I ...
Carry your important items in a pocket
DEAR HELOISE: I read a hint about what a lady did with her purse when she went shopping. I wanted to add one ...
Bridge by Steve Becker
TO YOUR GOOD HEALTH: Patient’s height is too often overlooked
DEAR DR. ROACH: Why is it that when one sees the doctor, the nurse will take their weight and blood pressure but ...